Condition
Tennis & Golfer's Elbow
Pain at the outside (tennis elbow) or inside (golfer's elbow) of the elbow from irritation of the forearm tendon attachments.
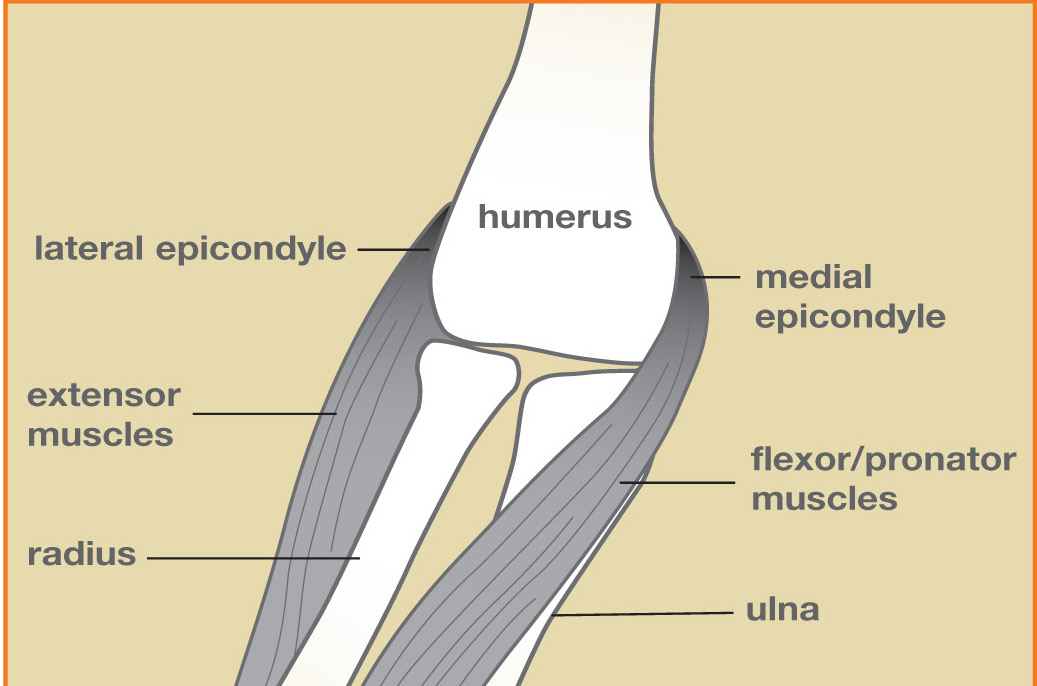
Illustration © American Society for Surgery of the Hand
What is tennis and golfer's elbow?
The forearm muscles that move your wrist and fingers attach at two small bony points on the elbow. The outside point is called the lateral epicondyle, and the inside point is the medial epicondyle. When the tendons that attach to these points become irritated, the result is pain at the elbow that is worse with gripping, lifting, and twisting.
- Tennis elbow (lateral epicondylitis) is pain on the outside of the elbow.
- Golfer's elbow (medial epicondylitis) is pain on the inside of the elbow.
Despite the names, most people with either condition do not play the sport. Everyday gripping, typing, carrying, and lifting are more common triggers.
Common symptoms
- Pain and tenderness at the bony point on the outside or inside of the elbow
- Pain when gripping, shaking hands, turning a doorknob, or lifting a coffee cup
- A weak grip or pain that travels down the forearm
- Stiffness and soreness first thing in the morning
Why does it happen?
Epicondylitis is an overuse condition. Small strains in the tendon attachment fail to heal normally and slowly build into a painful, chronic irritation. Common risk factors include:
- Jobs or hobbies that require repetitive gripping, wrist motion, or lifting
- Sudden increase in activity, especially a new sport or a home project
- Age between 35 and 55, when tendons lose some elasticity

Illustration © American Society for Surgery of the Hand
Treatment options
Good news: about 90% of people get better without surgery. Recovery is often measured in months, not weeks.
Non-surgical treatment
- Activity modification. Taking a break from the activity that triggers the pain, or changing how you grip, is often the most important step.
- Anti-inflammatories and ice. Over-the-counter ibuprofen or naproxen can help, along with ice after activity.
- Counterforce strap or wrist brace. A padded strap below the elbow or a rigid wrist splint can offload the irritated tendon and give immediate relief for many patients.
- Hand therapy. Eccentric stretching and strengthening, guided by a therapist, is the most effective non-surgical treatment and is usually done for 6 to 8 weeks.
- Steroid injection. A corticosteroid injection can reduce pain in the short term. It is usually reserved for stubborn cases because the effect often wears off after a few months.
Surgical treatment
- Tendon debridement. If pain has been present for 6 to 12 months despite good non-surgical treatment, a small outpatient surgery can remove the scarred, irritated tissue from the tendon attachment. Most patients have good or excellent pain relief, though full recovery takes several months.
What to expect at your visit
Dr. Barrera will examine the elbow, pinpoint the tender spot, and test which motions reproduce your pain. Imaging is usually not needed for a typical case, but X-rays or an ultrasound may be obtained if the diagnosis is unclear. Together you will build a plan that almost always starts with activity changes, a brace, and a short course of therapy.
Call us if the elbow becomes red, hot, or very swollen, if you have numbness or tingling radiating into the hand, if the pain is from a single sudden injury rather than gradual overuse, or if you cannot straighten or bend the elbow normally.
Related
Questions?
Call your office location for non-urgent questions:
- NYU Langone Laurelton · 646-501-4950
- NYU Orthopedic, Woodside · 929-429-3222
- NYU Orthopedic, Richmond Hill · 718-206-6923
- Jamaica Hospital Ambulatory Care Center (ACC) · 718-301-0720
See our office contact information for addresses and fax numbers.