Condition
Scaphoid Non-Union
A scaphoid fracture that has failed to heal. Left untreated, it leads to wrist arthritis. Treatment depends on where the non-union is and whether the bone has lost its blood supply.
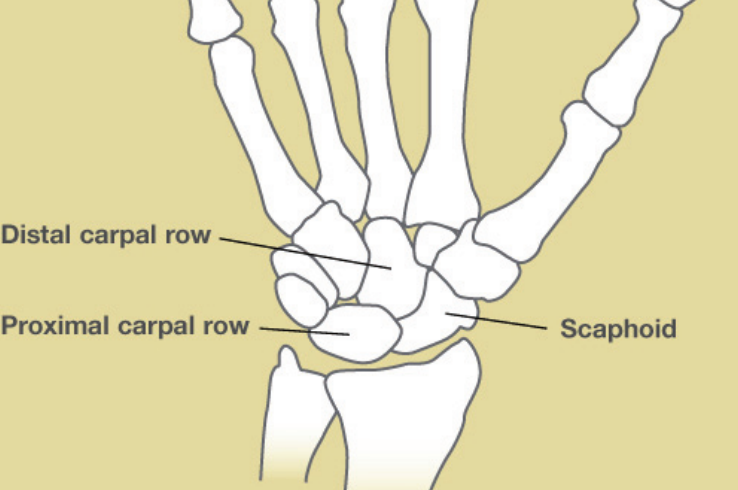
Illustration © American Society for Surgery of the Hand
What is a scaphoid non-union?
A scaphoid fracture that does not heal within about six months is called a non-union. Some non-unions happen because the injury was never recognized as a scaphoid fracture and was treated as a simple "sprained wrist." Others happen despite correct early treatment, because the scaphoid has an unusually fragile blood supply. The bone's blood vessels enter from the thumb-side end, so the wrist-side end (the proximal pole) depends on flow traveling across the fracture. When the fracture cuts off that flow, the proximal fragment can lose its blood supply entirely — a condition called avascular necrosis.
A scaphoid non-union is a distinct problem from a fresh scaphoid fracture. The bone has often shifted into a bent position (called a "humpback deformity"), the surrounding cartilage may be starting to wear, and ordinary healing methods no longer work. Without treatment, a non-union almost always leads to a predictable pattern of wrist arthritis over years.
Common symptoms
- Wrist pain on the thumb side that never fully went away after an old injury
- A weak grip or pain with pushing up from a chair
- Clicking or catching in the wrist
- Loss of wrist motion, especially extending the wrist backward
- Sometimes no symptoms at all — the non-union is found on an X-ray taken for another reason
Why does it happen?
- A missed or late-treated fracture. Scaphoid fractures are often dismissed as "sprains" and can be invisible on early X-rays. Weeks or months of use without a cast prevent healing.
- Fracture location. Breaks near the wrist-side end of the scaphoid (the proximal pole) heal slowly because blood has to cross the fracture to reach that fragment. These are the fractures most likely to fail even with correct treatment.
- Displacement. A fracture that was shifted or angled is much less likely to heal in a cast alone.
- Smoking. Nicotine narrows small blood vessels and is one of the strongest modifiable risk factors for a non-union.
- Other factors. Diabetes, chronic steroid use, and poor nutrition all slow bone healing.
Treatment options
The right operation depends on three questions: where in the scaphoid the non-union is, whether the proximal piece still has a blood supply, and whether the wrist has started to develop arthritis. An MRI and sometimes a CT scan are used to sort this out.
Non-surgical treatment
Surgery is not always required. Some older, painless non-unions discovered incidentally can be watched. Activity modification, bracing, and anti-inflammatories can control symptoms in patients who are not good surgical candidates. These options will not heal the bone, but they can be the right choice in selected patients.
Surgical treatment — healing the bone
- Non-vascularized bone graft with screw or plate fixation. For many non-unions with preserved blood supply, a graft of bone taken from the distal radius or the hip is placed into the non-union site and the scaphoid is fixed with a small screw, or in some cases a small plate. This is a reliable, well-established operation and is the right choice for most standard non-unions.
- Local (pedicled) vascularized bone flap. A small piece of bone is taken from the distal radius with its own blood vessels still attached and rotated into the non-union site. Because the flap never leaves the forearm, no microsurgery is required. This is a good option for selected non-unions, particularly in the waist or distal pole of the scaphoid when the proximal pole still has a reasonable blood supply.
- Vascularized bone flap from the knee (free flap). When the proximal pole has lost its blood supply, or when a previous operation has failed, a bone flap with its own blood vessels is often needed. A small piece of bone is taken from the inner side of the knee and connected under the microscope to blood vessels at the wrist. Two different flaps are used depending on where the non-union is:
- MFC (medial femoral condyle) flap — used for non-unions in the waist or body of the scaphoid. The MFC flap brings living bone and its own blood vessels to the non-union site.
- MFT (medial femoral trochlea) flap — used for proximal pole non-unions with avascular necrosis. The MFT is taken from the cartilage-covered part of the knee, so it restores both living bone and a new joint surface.
Surgical treatment — when the wrist is already arthritic
If the wrist has already developed advanced arthritis from a long-standing non-union, rebuilding the scaphoid no longer helps. Salvage operations relieve pain by changing how the wrist moves. These include proximal row carpectomy (removing the row of small bones that includes the scaphoid) and partial wrist fusion. Which one fits best depends on the pattern of arthritis.
Not every scaphoid non-union needs a vascularized bone flap — a standard non-vascularized graft is the right choice for many patients, and for advanced arthritis a salvage procedure gives better long-term function. However, for proximal pole non-unions with avascular necrosis, or for failed prior surgeries, vascularized bone flaps from the knee (MFC and MFT) can be the difference between healing the scaphoid and losing it. These are specialized reconstructions performed at only a small number of hand surgery practices. Dr. Barrera has fellowship training in these techniques and offers them when they are the right fit for the injury.
What to expect at your visit
Dr. Barrera will review your history, examine your wrist, and look at any prior X-rays you have. Additional imaging — usually an MRI to assess the blood supply of the proximal fragment, and sometimes a CT scan to look at bone shape and early arthritis — is often needed to decide the best operation. You will leave the visit with a clear plan and a frank discussion of what each treatment option can and cannot do.
Call the office if wrist pain after an old injury has been ignored and is getting in the way of work or sleep, if grip strength has suddenly dropped, or if a previous wrist surgery for a scaphoid fracture has not felt right. Earlier treatment of a non-union gives more options and a better chance of saving the joint.
Related
Questions?
Call your office location for non-urgent questions:
- NYU Langone Laurelton · 646-501-4950
- NYU Orthopedic, Woodside · 929-429-3222
- NYU Orthopedic, Richmond Hill · 718-206-6923
- Jamaica Hospital Ambulatory Care Center (ACC) · 718-301-0720
See our office contact information for addresses and fax numbers.