Condition
Brachial Plexus Injury
Damage to the network of nerves between the neck and shoulder that controls the muscles and feeling in the arm and hand.
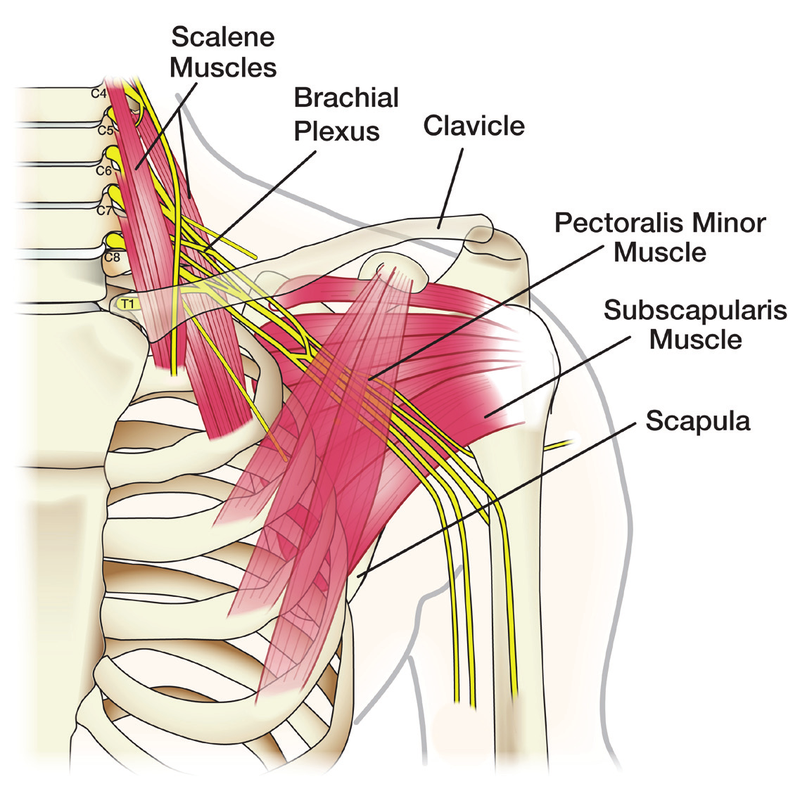
Illustration © American Society for Surgery of the Hand
What is a brachial plexus injury?
The brachial plexus is a group of nerves that come from the spinal cord in the neck, travel under the collarbone, and branch out into the arm. These nerves send signals from the brain to the muscles in the shoulder, arm, and hand, and they carry feeling back from the skin. An injury to the brachial plexus can cause weakness, loss of sensation, or paralysis of part or all of the arm. Injuries range from mild stretch injuries that recover in weeks to severe tears that require surgery to restore function.
Common symptoms
- Weakness or complete loss of movement in the shoulder, arm, or hand
- Numbness or loss of feeling down the arm
- Burning, electric, or stabbing pain in the arm
- An arm that hangs limp at the side
- A hand that cannot grip or fingers that will not move
Why does it happen?
The brachial plexus can be hurt by stretching, compression, or tearing of the nerves. The most common causes are:
- High-speed trauma. Motorcycle crashes, car accidents, and falls are the most common cause in adults. The shoulder is pushed away from the neck, stretching the nerves.
- Direct impact or crush. A heavy blow to the side of the neck or shoulder, or a shoulder dislocation, can compress or tear the nerves.
- Sports injuries. Contact sports can cause a "stinger" or "burner" — a temporary stretch injury that usually recovers quickly.
- Gunshot or stab wounds. These can directly cut part of the plexus.
- Tumors or radiation. Less commonly, tumors or scar tissue from radiation can compress the nerves.
- Birth injury. The brachial plexus can be stretched during a difficult delivery.
The severity depends on whether the nerves are stretched but intact, partially torn, completely torn, or pulled off the spinal cord. This distinction determines whether recovery is expected with time alone or whether surgery is needed.
Treatment options
Non-surgical treatment
- Observation and hand therapy. Mild stretch injuries often recover on their own over weeks to months. Therapy keeps the joints moving and the muscles ready to work again once the nerves heal.
- Pain management. Brachial plexus injuries can cause severe nerve pain. Medications used specifically for nerve pain, along with therapy, are part of the plan.
- Splinting. A sling or custom splint protects the shoulder and helps prevent stiffness during recovery.
- Nerve studies. An electromyogram (EMG) and nerve conduction study are usually done at 3 to 4 weeks, and sometimes again later, to tell how badly the nerves are hurt and whether they are starting to recover.
Surgical treatment
The timing of surgery matters. Nerves heal very slowly, and muscles that lose their nerve supply begin to permanently atrophy after 12 to 18 months. When surgery is needed, it is usually done within the first several months after injury to give the best chance of recovery.
- Nerve exploration and repair. If a nerve is cut, the two ends are sewn back together under a microscope.
- Nerve grafting. If a segment of nerve is missing or damaged, a small sensory nerve from the leg can be used as a bridge.
- Nerve transfer. A working nerve that does a less important job is rewired to take over the job of a more important nerve that is not recovering. This is often the best option for restoring shoulder and elbow function.
- Tendon and muscle transfers. Later in recovery, a working muscle can be moved to substitute for a muscle that is no longer working.
- Free functioning muscle transfer. In severe cases, a muscle from another part of the body is transplanted and reconnected using microsurgery to restore specific movements.
What to expect at your visit
Dr. Barrera will take a detailed history of the injury, examine the shoulder, arm, and hand to test every muscle group, and check the feeling in each nerve area. An EMG and nerve conduction study, MRI of the brachial plexus, or CT myelogram may be ordered to tell which nerves are injured and how severely. Together you will build a plan that combines therapy, nerve studies, and — if needed — a carefully timed surgery. Brachial plexus recovery is a long process measured in months and years, not weeks, and a coordinated team including hand therapy and pain management is part of the care.
Call us if there is new weakness in the arm or hand, new numbness that is not getting better, severe or worsening nerve pain, signs of infection at a surgical site, or if you feel the arm is becoming stiff or cold and pale.
Related
Questions?
Call your office location for non-urgent questions:
- NYU Langone Laurelton · 646-501-4950
- NYU Orthopedic, Woodside · 929-429-3222
- NYU Orthopedic, Richmond Hill · 718-206-6923
- Jamaica Hospital Ambulatory Care Center (ACC) · 718-301-0720
See our office contact information for addresses and fax numbers.