Condition
Cubital Tunnel Syndrome
Compression of the "funny bone" nerve at the elbow. Causes numbness in the ring and small fingers and can weaken the hand.
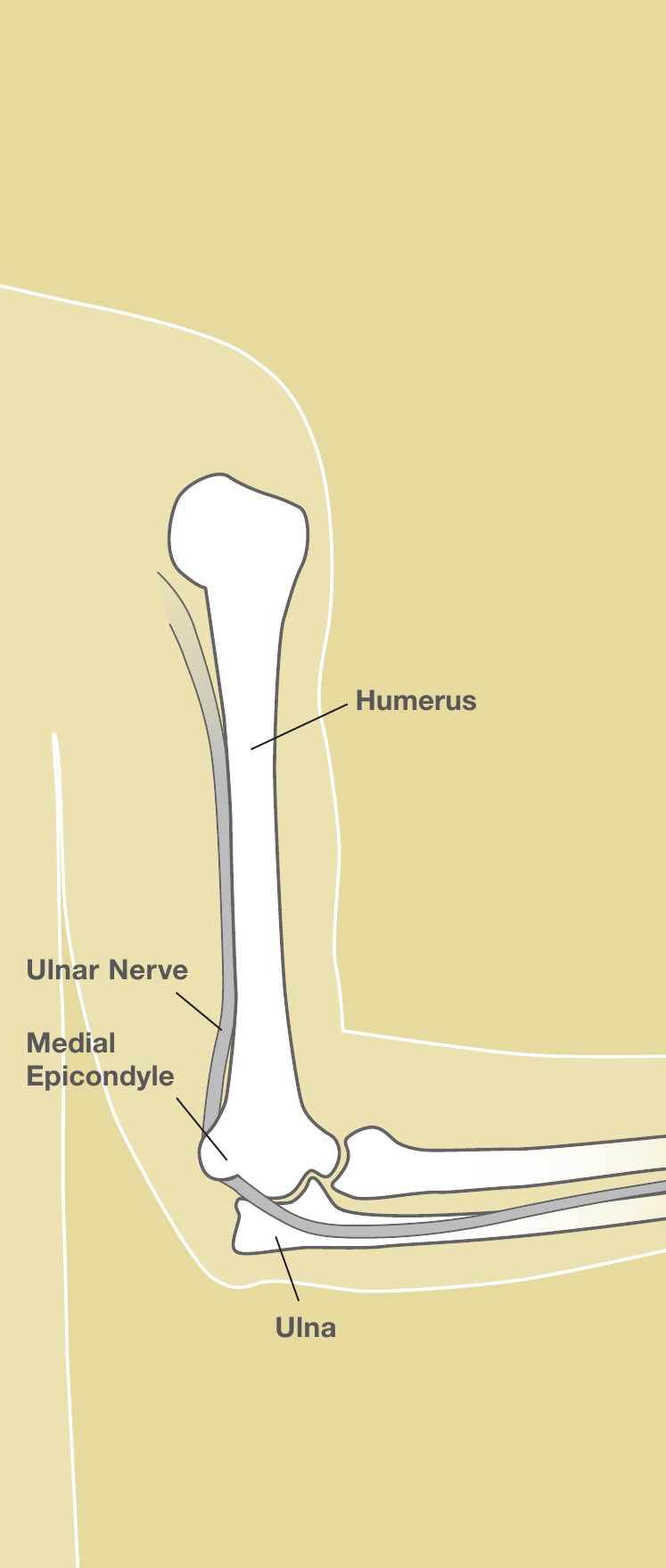
Illustration © American Society for Surgery of the Hand
What is cubital tunnel syndrome?
The ulnar nerve runs from the neck down the arm and passes behind the inside of the elbow through a narrow tunnel called the cubital tunnel. It is the nerve you feel when you bump your "funny bone." When the tunnel is tight or the nerve is stretched, numbness, tingling, and weakness develop in the hand.
Common symptoms
- Numbness or tingling in the ring and small fingers
- Symptoms that are worse when the elbow is bent, for example while holding a phone or sleeping
- An achy feeling along the inside of the elbow or forearm
- Weakness in grip, difficulty spreading the fingers, or trouble crossing the fingers
- Loss of muscle bulk between the thumb and index finger in long-standing cases
Why does it happen?
Bending the elbow stretches the ulnar nerve and narrows its tunnel. Anything that keeps the elbow bent for long periods, or direct pressure on the inside of the elbow (such as leaning on a desk or armrest), can cause symptoms. Some people have anatomy that makes the nerve slide out of place when the elbow bends, which can irritate it over time.
Treatment options
Non-surgical treatment
- Activity changes. Avoid leaning on the inside of the elbow. Use a headset instead of holding a phone to the ear.
- Nighttime splint or elbow pillow. A soft splint or a towel wrapped around the elbow keeps it mostly straight while you sleep. This alone resolves symptoms for many people.
- Therapy. Nerve-gliding exercises and posture changes can help early cases.
Surgical treatment
- Cubital tunnel release. A short outpatient surgery releases the tight tissue over the nerve at the elbow.
- Ulnar nerve transposition. In some patients the nerve is moved to the front of the elbow so it does not stretch with bending. Dr. Barrera will discuss which option fits your anatomy.
What to expect at your visit
Dr. Barrera will examine your elbow and hand, test sensation and strength, and look for muscle wasting. Most patients get a nerve study (EMG) to confirm the diagnosis, measure severity, and rule out compression elsewhere along the nerve. Imaging is sometimes useful if there has been a prior elbow injury.
Call us if your grip is rapidly getting weaker, if you notice the muscles in your hand starting to waste, or if you cannot bring your fingers together. Long-standing severe nerve compression is harder to reverse, so earlier treatment tends to work better.
Questions?
Call your office location for non-urgent questions:
- NYU Langone Laurelton · 646-501-4950
- NYU Orthopedic, Woodside · 929-429-3222
- NYU Orthopedic, Richmond Hill · 718-206-6923
- Jamaica Hospital Ambulatory Care Center (ACC) · 718-301-0720
See our office contact information for addresses and fax numbers.